72 yr old male patient with shortness of breath
A 72 year old male patient presented with the chief complaints of :
S.O.B since 15 days
decreased urine output since 10 days
pedal oedma since 10 days
History of presenting illness:
Pt was apparently asymptomatic 14 years back then in 2008,he developed slurred speech and an abnormal gait for which he was taken to a neuro surgeon where he was managed conservatively for a week and was an medication for 4 years . ( medication unknown, indication unknown)( possibly stroke).at the same time he was known to have HTN and is on medication since then.
Then after 4 years ,in 2012 ,he was having severe SOB and was taken to a hospital where he was diagnosed with COPD and the medication dose was decreased and his symptoms subsided.
In 2018 , then he had a trauma to the leg which was not healing and was taken to thehospital where rountine check up was done to find to have Type 2 DM .
Then in 2021 he developed bilateral pedal edema and on investigations it was found that CREATININE was high and diagnosed as CKD
and Now he presented with the SOB (grade 3) since 12-15 days. Grade 4 since 3 days.i.e.,( SOB on rest)
Pt has fever since 3 days.
not associated with palpitations, sweating
loss of appetite since 15 day
decreased urinary output since 10 days
No history of hematuria, burning micturition.
Bilateral pitting type of pedal edema since 10 days
he was taken to a local hospital where they found to have higher creatinine and was sent here for further management.
Past history:
HTN since 14 years and on medication since then
DM since 4 years and on medication
known case of CKD since 2 years
no history of TB ,Asthma ,CAD
Personal history:
Diet - mixed
appetite - decreased
bowel and bladder - Regular
sleep - adequate
Addictions - smoked for 15 years and stopped smoking after diagnosed with COPD in 2012 .
occasionally alcohol
Family history:
No relevant family history
Allergic history:
no allergies for any kind of drugs and food.
GENERAL EXAMINATION:-
patient was semi - conscious and is on ventilator
Not so well nourished and weakly built.
VITALS:-
Temperature:- febrile
P.R :- 100
R.R :- 24
BP :- not measured
GRBS :- 177mg%
Pallor +
icterus -
cyanosis -
clubbing -
lymphadenopathy -
Bilateral pitting type of edema +







SYSTEMIC EXAMINATION:-
RESPIRATORY SYSTEM:-
INSPECTION:-
Antero - posterior diameter increased (barrel shaped chest).
on inspection and palpation:- Trachea is central
AUSCULTATION:-
Bilateral air entry present .
FINE CREPTS are heard at
right and left infra axillary and right and left infra scapular areas
CARDIO VASCULAR SYSTEM:-
S1 ,S2 heard
No Murmurs heard
PER ABDOMEN:
shape of abdomen:- Scaphoid
no tenderness
no palpable organs
bowel sounds - present
CENTRAL NERVOUS SYSTEM:-
patient is semi conscious .
Signs of meningeal irritation:- -ve
cranial nerves - not done
sensory system - not done
motor system - not done
Investigations:
Random blood sugar
Taken on 31/7/22


RFT 1/8/22

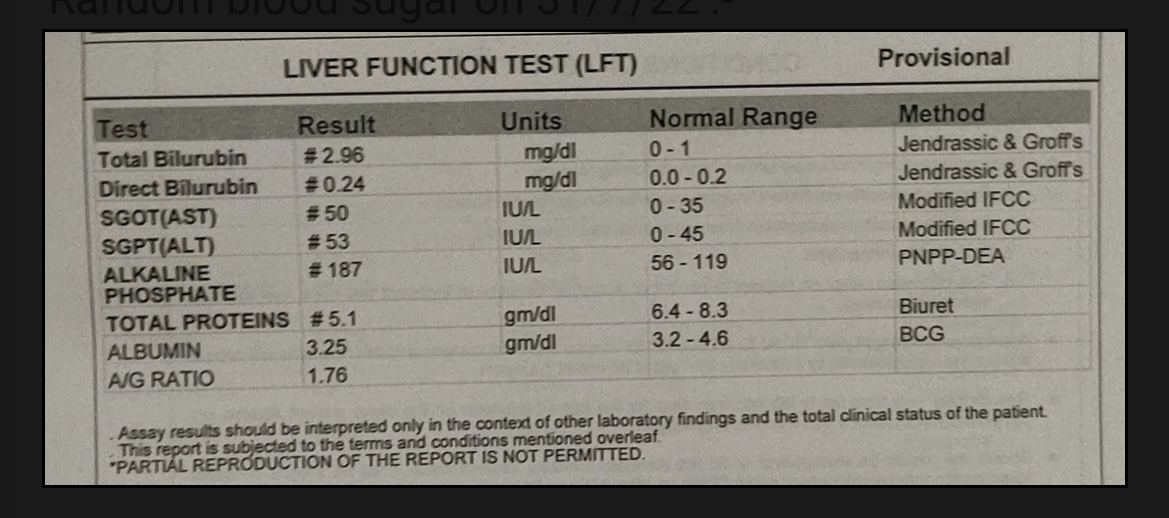
LFT 1/8/22




HEMOGRAM:

SEROLOGY:



ECG 1/8/22

ABG 31/7/22

ABG 1/8/22

ABG 2/8/22




X-RAY ON 2/8/22

DIAGNOSIS:-
Acute excerbation of COPD.
CKD secondary to diabetic nephropathy
Anemia of chronic disease
PLAN OF CARE :- Supportive management
TREATMENT:-
1) Fluid restriction less than 2L/day
2)Salt restriction
3) NEB - DUOLIN 8 th hrly
BUDECOID 12 hrly
4) I.V PIPTAZ 2.25 gm IV BD
5) I.V PAN 40 mg BD
6)LASIX 60 mg IV BD
7) HYDRO CORTI 100 mg
8) INJ NEOMOL 1g IV
9)INJ LEVOFLOX
10)INJ ERYTHROPOIETIN 4000 IU
11) T Shelcal 500 mg
12)NODOSIS 500 mg
13) GRBS charting 6 th hrly
14) vitals charting 4 th hrly



Comments
Post a Comment